The nerves that produce orgasm are not as most men think just in the clitoris, but there are a variety of nerves that lead from the spinal cord to areas of pleasure.
At BioBalance we treat sexual dysfunction in both men and women with testosterone and 90% of the time, it works well, bringing women’s desire and sexual function back to what they experienced as young women.
Before I specialized in hormone replacement bio-identical pellets, I struggled with the treatment of the female problems of anorgasmia, painful intercourse from pelvic diseases like endometriosis, and pelvic pain from menopause. Unfortunately, as a gynecologist I was given one day of training about female sexual function and dysfunction during my residency. This was 99% too little training for the only doctors expected to advise women in the US about sex and sexuality!
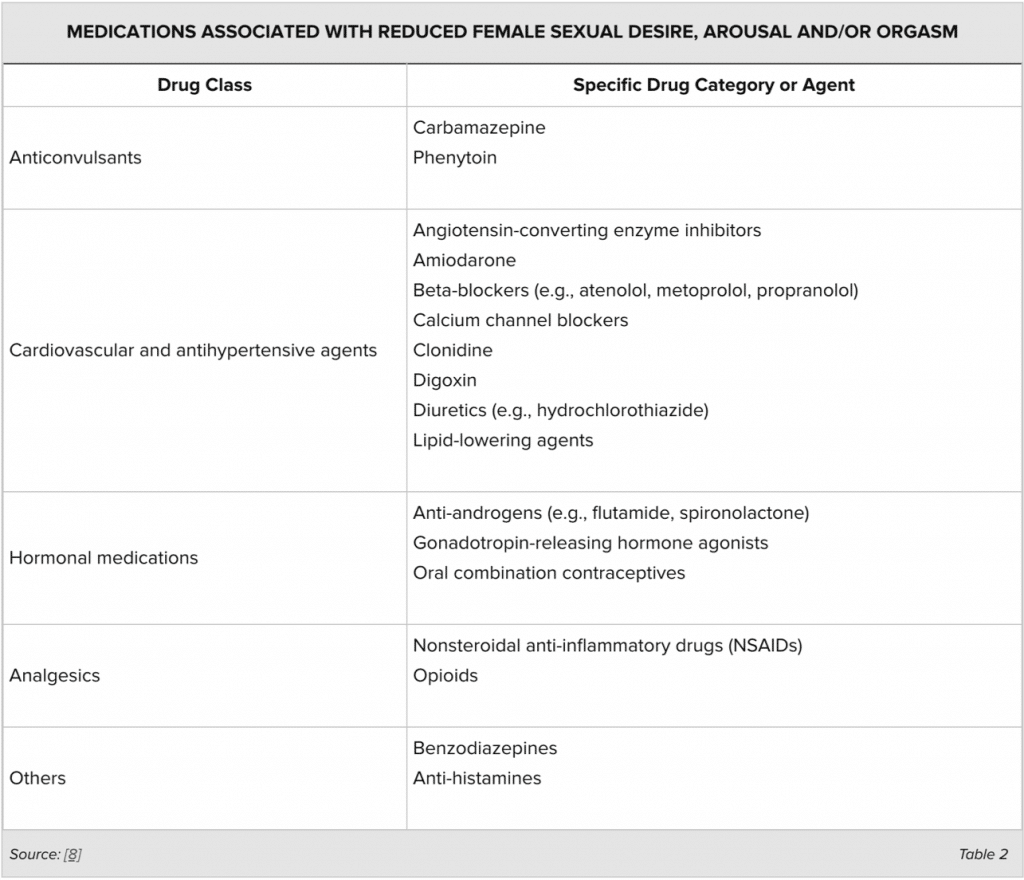
I have had extra training in sexuality now, and I talk about sex all the time when working with premenopausal and menopausal women. The biggest problems I deal with are lack of sex drive, poor or non-existent orgasms, painful intercourse from lack of vaginal lubrication and deep pain from pelvic endometriosis, fibroids, and intra-abdominal scarring. Because of my work with hormone replacement, I found that 90% of female dysfunction is due to low testosterone and or estrogen. The rest is caused by past sexual abuse, side effects to medications, past surgeries, diseases that involve the nerves of the pelvis, diseases or surgeries that cause adhesions in the pelvis and other diseases that compromise the normal blood flow to the female pelvis.
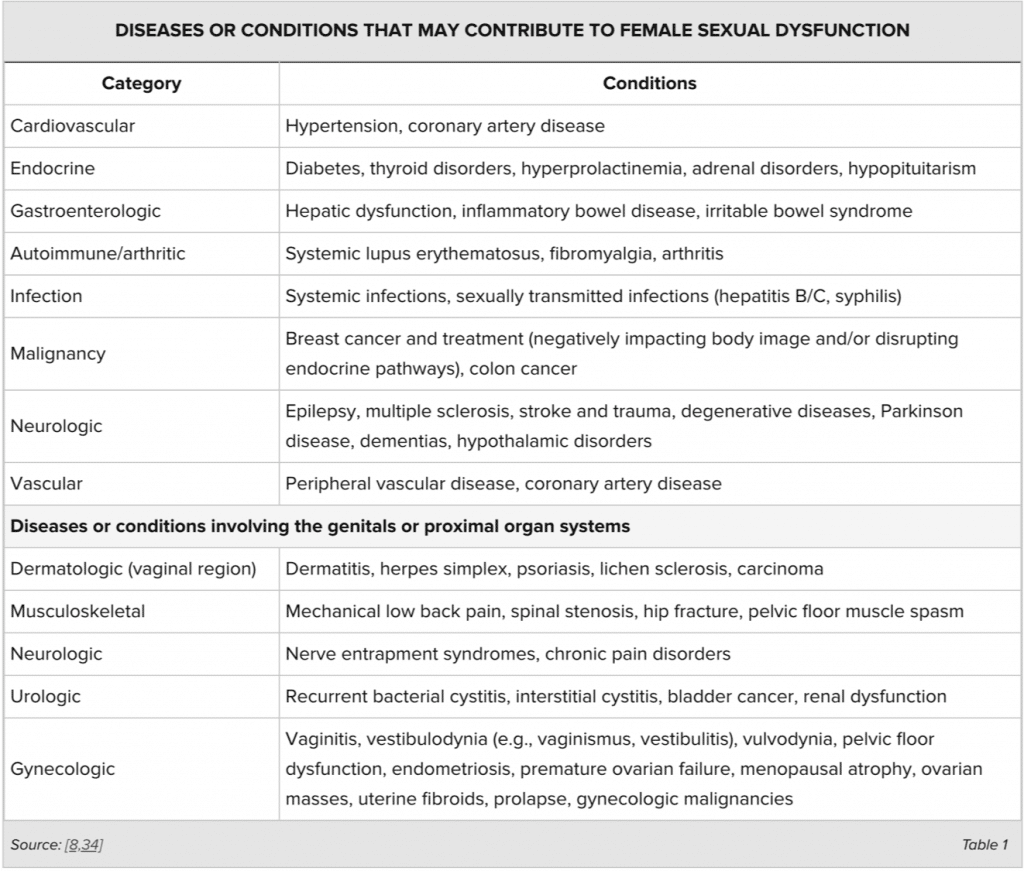
If you look at this chart, Sex Hormones occupy 90% of the causes of female sexual dysfunction in women and everything else takes up only 10%.
First a word about sex and anatomy. Basically, the uterus is an organ suspended in the pelvis by 2 sets of ligaments that allow it to move up and down and sideways when there is sexual penetration. The uterus can move away from direct pressure on the uterus, and the vagina stretches to a length about 8 inches to accommodate the largest penis. Both vaginal length and penis size is genetic and there are big differences between races.
Back to the sex act and anatomy. When there is maximum penetration, the uterus moves toward the head and the abdominal organs move away from the uterus to accommodate the extra volume that the penis adds to the contents of the abdominal cavity. If there is no pelvic mass like a fibroid to bump into or adhesions from surgeries holding the uterus in place so it can’t move into the abdomen and make room for the penis, then there will be pain. When anything in the abdomen including the pelvis is held in one position the movement necessary for the intestines or for intercourse causes pain when it hits the paralyzed organ.
With a uterus that has become stuck by adhesions or endometriosis, deep thrust during intercourse feels like being rammed with a hot poker when the penis hits the cervix. In these cases, not thrusting up to the cervix sometimes does the trick or changing the position of intercourse so the woman is on top and can dismount if it hurts too much.
In women who have no impingement to the movement of the uterus and cervix, the movement of the cervix s pleasurable and can cause a deep climax that is different than those produced by stimulating other areas. Let me insert this bit of important information—if the vagina is dry from low dose birth control pills or menopause without estradiol or testosterone replacement, there is no amount of cervical movement that will feel good enough to end in an orgasm.
There is currently no treatment for the problem of pelvic adhesion or fibroids, ovarian cysts or a retroflexed uterus besides hysterectomy or laparoscopy to remove adhesions. My advice in this case is that if a hysterectomy is necessary, then have your doctor leave the cervix so you can once again enjoy cervical orgasms. It is necessary for the doctor to leave the cervix and the ligaments that hold it up but core out the lining of the cervix, so you don’t bleed when replaced with estrogen.
The nerves that produce orgasm are not as most men think just in the clitoris, but there are a variety of nerves that lead from the spinal cord to areas of pleasure. One nerve group leads to the opening of the vagina and the labia, so that manipulation of this area can bring on an orgasm. Another is at the clitoris as expected, a third goes through the uterine ligaments that leads to the cervix and are stimulated by movement. A fourth is located at the opening of the rectum. The G spot is an area of great doubt to the common man, but it does hold the nerves that are located around the prostate in a man, and to the G spot in a woman. This spot is on the top of the vagina about 1.5 inches from the opening. It feels like a small mound of tissue and is different in character than the tissue around it. I taught many women to find their own G spot, so they could teach their partners where it was, and we had great success. The rumor that it is a figment of a woman’s imagination is exaggerated.
This Health cast was written and presented by Dr. Kathy Maupin, M.D., Bio-identical Hormone Replacement Expert and Author, with Brett Newcomb, MA., LPC.,Family Counselor, Presenter and Author. www.BioBalanceHealth.com.
