The sexual areas meant to be stimulated to bring a woman to orgasm are in the pelvis and breasts.
Warning: I will be discussing the female anatomy and sexual responses in this healthcast, so you may want to listen to this and the next few healthcasts in a private location. I will use correct anatomical labels for sexual organs and sexual responses Like I do with my patients in my office.
The first step in understanding how your sexual organs work and how you can have an excellent and gratifying sex life is to understand the anatomy of the sexual organs and what each organ works. The pelvis, vagina, and perineum are the primary areas of stimulation to bring a woman to orgasm. There are other areas, primarily the breasts and other erogenous areas that can bring on an orgasm. The sex organs are where the stimulation starts but the brain is where the actual orgasm takes place and the production of neurotransmitters called endorphins is the outcome of the stimulation and the goal of having sex—the feel-good brain hormone that makes women feel warm and attached and excited as well as the chemicals that bring on sleep and can relieve pain and anxiety. The phrase that sex is all in your head is actually true!
The sexual areas meant to be stimulated to bring a woman to orgasm are in the pelvis and breasts. We will address the pelvis in this Health cast. The female reproductive anatomy is divided into three areas of the pelvic area, all located below the belly button. The Perineum, the Vagina and the Internal Pelvic Organs. The perineum is located on the outside of the vagina, that area you can easily see by using a mirror and looking at the area around the outside of the vagina between a woman’s legs. It includes the Mons, clitoris and clitoral hood, urethra, periurethral glands, vaginal opening, labia minora, labia majora and the anus. The Vagina is the area inside the opening of the vaginal, the hymenal ring and includes the cervix, vagina itself, and G-spot. The third area is called the internal pelvic organs and is located inside the abdomen below the belly button, and includes the uterus, ovaries, and fallopian tubes. You can’t see these organs without an invasive procedure like a laparoscope or a radiologic procedure like an ultrasound of the pelvis. Gynecologists use palpation (feeling the organs through the vagina and abdominal wall) to estimate the size and shape of these organs. This particular part of the gyn exam is how we can diagnose uterine fibroids, ovarian cysts and masses and adhesions as well as other pathology without using an ultrasound.
First the external reproductive area, the perineum, is loaded with nerves from many different areas on the lower spinal cord. In other words, different parts of the female perineum have different nerves for sensation that connect with the spine in a variety of areas, that can all transmit information to the brain. All of these nervous connections can stimulate the release of endorphins and produce an orgasm. Different areas of stimulation produce specifically unique orgasmic feelings, and women with a great deal of sexual experience can tell which orgasm comes from which area of stimulation, and they can actually have several types of orgasm at the same time if several areas are stimulated at the same time!
The Perineum:
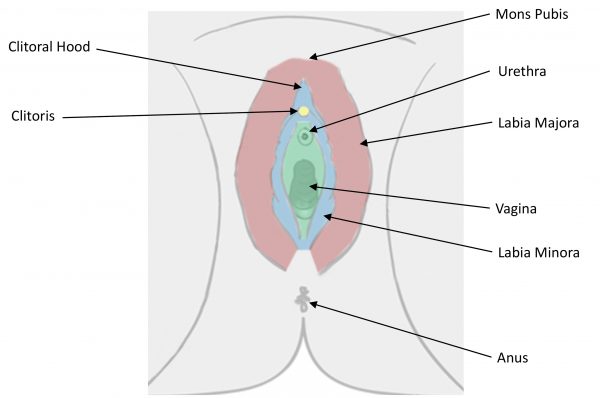
This is a schematic picture of the perineal anatomy. The most important sexual area is the clitoris, which has many nerves and blood vessels coming to and from it. It is the clitoris that provides the primary orgasm for the majority of women, so it is important that you know where it is, and know that it normally swells with stimulation, either manual or oral, and the hood that normally protects it, pulls back and exposes the clitoris so it is more available to further stimulation. Stimulation causes the clitoris to enlarge and become firm, similar to the male penis. In certain sexual positions the clitoris can be stroked by the penis, otherwise it can be stimulated by tactile stroking, and oral stimulation.
The mons is the fat pad above the clitoris that protects a woman’s pubic bone, and her partner’s from being bruised during long sessions of sexual intimacy. The mons acts as padding during sex and can be sensitive to touch during foreplay and tactile stimulation. On the lateral areas around the vagina are the Labia Majora, or the hairy labia. They swell with sexual stimulation and act as shock absorbers. The labia that do not grow hair are called the labia minora. There is much controversy about these labia. The “sexual-beauty experts” have decided that the labia minora typical for women who are genetically from northern Europe and Asian are the “most beautiful” which is an artificial assessment. This trend made women worry about the size of their labia and many women have had plastic surgery to remove large labia minora. The longer or larger labia minora are characteristic of southern Europe and African genetically. Interestingly, larger labia minora are genetic adaptations to accommodate larger male penises. Larger labia minora lengthen the physical length of the vagina to accommodate larger penises. Your labia minora have many sensory nerves which are beneficial to being orgasmic, so my advice is, don’t “hate” them because they are large, remember that the more sensation, the better the sex!
If a woman is sitting in lithotomy, like at the gyn’s office with her knees up, heels close to her buttocks with her knees spread apart, the mons is toward the ceiling, the clitoris is below the mons, and the urethra, the opening to bladder comes next, below the clitoris. The urethra is very sensitive and can be a source of pleasure, but it must be treated with gentleness. There are two tiny openings on either side of the urethra called the Periurethral glands. They are hard to see, but they are openings to glands that supply lubrication for sex. These glands are one of the producers of ejaculate in women. Some women do ejaculate and some of the fluid comes from the periurethral glands, some comes from the vaginal wall which can secrete al large amount of fluid at orgasm. Both the vagina and the periurethral glands produce female ejaculate, and it is not urine! The ability to ejaculate depends on the amount of testosterone a woman has, how effective sexual stimulation is and how good the orgasm is.
Below the urethra and periurethral gland openings is the vaginal opening. Prior to first intercourse there is usually a tight circular band around the vaginal opening. This band is called the hymenal ring and is broken at the first intercourse. The vagina itself has very thick lining when women are fertile adults, until they go through menopause when the vaginal skin becomes very thin and fragile from lack of estradiol. Young women’s vaginal tissue is stretchy enough to accommodate any size penis and it can stretch under the influence of pregnancy hormones, enough to deliver a baby! Most vaginas in women of fertile age are 2 fingers wide at rest and wider when simulated. Childbirth without episiotomy can stretch the vaginal opening much larger, and sometimes surgical repair is needed after childbearing to tighten the vaginal opening enough for intercourse.
The last area we will talk about on the perineum is the anus. The area around the outside the anus had a multitude of nerves that can be stimulated to achieve an orgasm. Aal sex is outside the scope of this healthcast. It takes special techniques and cleansing to successfully embark on this type of sexual activity.
Vagina
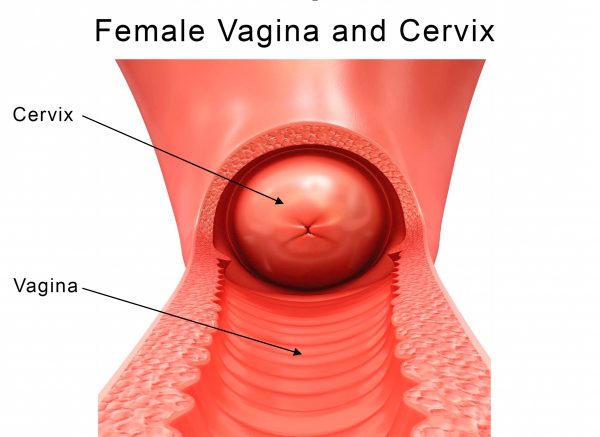
The vagina, the second anatomical area is about 4 inches long (deep), but lengthens with sexual stimulation, and childbearing. The vagina is a cave-like structure. Many of my patients think that at the top of the vagina is their intestines and it opens to the abdominal cavity, but that is not so. There is a tiny cervical canal that allows sperm into the uterus but in general, the vagina is a blind pouch or tunnel that ends in the cervix. Near the opening of the vagina on the wall of the vagina that is toward the ceiling when you are in lithotomy position, is the G-Spot, a thickened mound of vaginal tissue about 1-2 inches inside from the vaginal opening on the “ceiling of the vagina”. The G-spot is a site where stimulation can initiate an orgasm. It can be stimulated manually, or it can be stimulated by the penis from rear entry intercourse in the “doggie position “. It is thought to be a structure with the same nervous innervation as the male prostate.
The research of Beverly Whipple PhD., a research doctor who wrote the book “The G-Spot”, and The Orgasm Answer Guide, outlines in detail the areas of the perineum and vagina that lead to orgasms in specific areas in the brain. She did her orgasm research with Dr. Komasarek, her co-author. They studied women with an MRI machine and watched their brain activity while they masturbated until they achieved an orgasm. Their study revealed that self-stimulation can cause an orgasm that lights up the whole brain on the MRI. The lights represent the secretion of many neurotransmitters in every area of the brain. Before they did the study, they had expected that orgasms would light up one or two areas of the brain and they were surprised when orgasms lit up the whole brain! It confirms the belief that sex may begin in the pelvis, but orgasm is really located in the brain. For those of you who are physicians and want to learn more about orgasm, Dr. Whipple wrote a wonderful book called The Science of Orgasm which explains the details of orgasmic function and the whole neurologic pathway associated with orgasms.
The cervix is at the end of the vagina, and it has nerves that go to a different area of the spinal cord than the perineum, the vagina, the anus and the G-Spot. Stimulation of the Cervix creates a different kind of orgasm than the other areas. when stimulated through manual manipulation (with fingers) or when a penis or vibrator pushes the cervix back and forth or side-to-side. These are called cervical orgasms.
The Cervix has a tiny opening called the Endocervix that leads to the inside of the uterus. The cervix bridges the vagina and the abdominal pelvis. The cervix is actually the lower part of the uterus, but we physicians refer to it as if it is a different organ. It is the cervix that is tested with a pap smear to find cervical cancer.
Female Pelvis
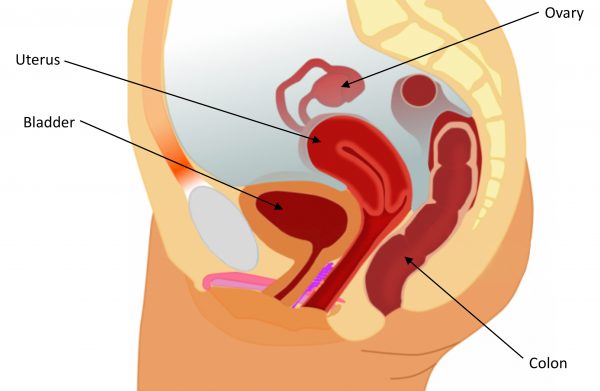
The Female Abdominal Pelvic Organs inside the abdomen include the Uterus or the “womb” where the baby grows in pregnancy, the Fallopian Tubes which are the tunnel that allows the ovum or egg to travel from the ovary to the inside of the uterus to be fertilized by sperm swimming from the vagina to the uterus, and the ovaries, which produce one or two eggs every month during the fertile years in preparation for pregnancy. The ovaries are producers of hormones Estradiol, Testosterone and Progesterone, and the uterus, vagina, and perineum are receivers of these hormones. The ovaries work from menarche (the first period) to Menopause (the last period) and then they stop working all together and shrink to a small fibrotic nubbin.
A hysterectomy means the removal of the uterus only. A total hysterectomy is removal of the uterus with the cervix. A supracervical hysterectomy is the removal of the uterus, leaving the cervix in place. I preferred the supracervical hysterectomy for my patients because by leaving the cervix in place I could preserve their orgasmic function. There are many women who have their uterus and cervix removed who feel that they are missing the cervical orgasms that they had before surgery, and I did not want that type of surgery for myself or for them.
The role the ovaries play in orgasms is just the production of estradiol and testosterone that together have sex and orgasmic function possible. Most of my patients come to me for replacement of testosterone because they lost their orgasms when they lost their hormones. No amount of stimulation or attention from their spouses can bring them back until they have their testosterone and estradiol replaced with bio-identical pellets.
A note about the uterus. The uterus plays very little part in sexual responsiveness unless the uterus is sick in some way. If the uterus develops fibroids and enlarges to any extent intercourse can cause pain when the penis moves the cervix. It can feel like the penis is slamming against the uterus and the uterus can’t move with the thrust. If there is endometriosis, there is pain with any kind of stimulation that causes blood flow to come to the pelvis. If the uterus is retroflexed which means angled backwards toward the rectum, during intercourse the penis pushes both the cervix and the top of the uterus at the same time. It is folded on itself so there is pain with intercourse. If everything inside the pelvis is healthy the uterus won’t interfere at all with sexual response, but it doesn’t contribute to it either. The good news is that if the uterus must be removed, and the cervix is left in place, there should be no change in sexual activity or sexual response. Orgasms should be the same and to the woman who had the supracervical hysterectomy, it feels like her uterus is still there!
Next week we will discuss the erogenous areas of the body and the most sensitive areas to stimulate to create orgasms. We look forward to a continued discussion on Sex and Women next week.
This Health cast was written and presented by Dr. Kathy Maupin, M.D., Bio-identical Hormone Replacement Expert and Author. www.BioBalanceHealth.com (314) 993-0963
