What is a vaginal ultrasound so important before starting hormone replacement therapy?
At BioBalance Health we use the information from a vaginal probe ultrasound, combined with information from your medical history questionnaire, and an extensive fasting blood panel to determine whether an individual woman is a candidate for estradiol and testosterone bioidentical pellets.
We also review the collated information to determine if we need more tests before we see a new patient.
The ultrasound of the pelvis gives us a visual picture of the ovaries and uterus of a woman. It is necessary to know if a patient is menopausal yet to interpret a new patient’s ultrasound. We obtain that information from your blood lab and medical history from the patient questionnaire. All three pieces of information are essential to our treatment plan.
What can we discover from the vaginal ultrasound?
We are ruling out (making sure a woman doesn’t have these pelvic problems):
Several of these conditions preclude the use of estradiol in any form, some require a visit to your gynecologist for treatment before we add estradiol to your hormones and some of these conditions increase the risk of side effects.
- Endometrial Cancer
- Endometrial hyperplasia
- Endometrial polyps
- Fibroids
- Ovarian cancer
- Ovarian cysts
- PCO
**We use the vaginal ultrasound to determine the risk of bleeding on HRT.
***For the first 3 uterine pathologies listed above we look at the measurement of the Endometrial Thickness (ET), or finding an endometrial polyp necessitates a visit to her GYN for evaluation, and most probably an endometrial biopsy or D&C. This pathologic test will rule in or out Endometrial cancer, endometrial hyperplasia.
The other diagnoses are determined by looking at the uterine size, contour, whether there are uterine fibroids, and looking at the ovaries for cysts or masses and the presence or absence of fluid in the cul-de-sac (area behind the uterus).
Why would we order a Vaginal Probe US for our hormone pellet patients after the first visit, while they are taking estradiol?
- Uterine bleeding is non-responsive to treatment
- Uterine size is getting larger (patient complains of pain or pressure)
- High risk patients with recurrent uterine bleeding
- To follow the growth of fibroids
- To check the ovaries in patients who have a Family History of ovarian cancer (generally we have the patient’s GYN follow this).
- To follow a benign looking cyst seen on the first US for growth.
What does the Vaginal US measure when they measure the endometrium?
ACOG guideline/Committee Opinion
US Endometrial thickness and other factors that trigger sending a woman to her GYN for tissue diagnosis.
The endometrial Thickness should be less than or equal to 4 mm (millimeter) after menopause if the woman is bleeding and less than 6 mm if she is postmenopausal and not bleeding.
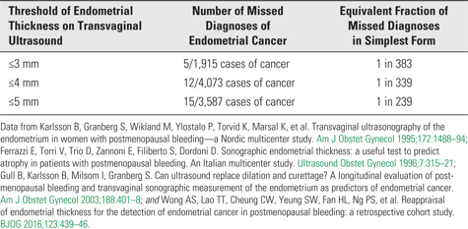
We usually will order an ultrasound in one of our established menopausal patients if she is bleeding and we can’t get it to stop with usual methods like increasing the progesterone dose. The following data is critical endometrial thickness measurements for women who are menopausal AND bleeding:
The guideline measurement of the Endometrial Thickness for Women WITHOUT BLEEDING, like we do on our New Patients = or < 6 mm
The utility of transvaginal ultrasonography to exclude pathology in postmenopausal women with bleeding should not be extrapolated to asymptomatic postmenopausal women without bleeding. In 1,750 postmenopausal women without bleeding who were screened for a selective estrogen receptor modulator study, an endometrial thickness of 6 mm or less had a negative predictive value of 99.94% for excluding malignancy (only one case of cancer in 1,750 women) and a 99.77% negative predictive value for complex hyperplasia (only four cases in 1,750 women). ACOG Committee Opinion
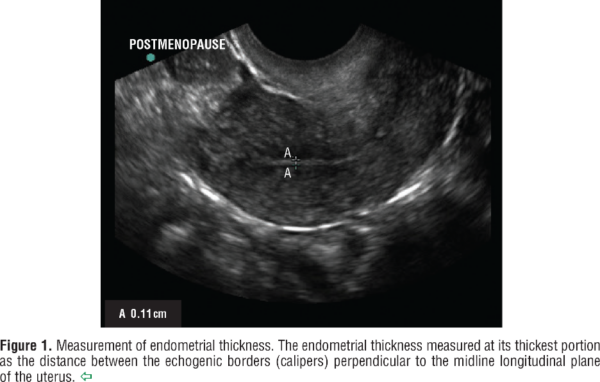
What is the Type of US needed to make a diagnosis? Transvaginal ultrasound is the only dependable type of ultrasound to determine this measurement. The measurement at the thickest point between the echogenic borders = endometrial thickness (ET) in mm.
WHEN to send a woman to her GYN for an endometrial biopsy, in our practice, is based on Stage of life-either Pre-menopause or Menopause, with bleeding (after the first US).
Note: Postmenopausal bleeding as an indication for an ultrasound if the uterine bleeding is resistant to treatment. Here is how we look at the endometrial thickness measurement from the vaginal probe ultrasound:
- ET> 4 mm on vaginal probe ultrasound greater than 4 mm in post menopause with uterine bleeding
- ET> 6 mm in Postmenopausal women without bleeding—like our New Patients on (Screening US)
- Premenopausal woman without bleeding > 16 mm (Screening US)
- Premenopausal woman with bleeding> 11 mm
- Presence of “abnormal findings” in the endometrial canal eg. Polyp, blood or trapped fluid anything called “suspicious” by the Radiologist
- Diagnosis of high risk factors with vaginal: Obesity, Type two diabetes, Polycystic Ovarian disease, history of other estrogen cancers, taking tamoxifen.
When do we send a woman to her GYN for biopsy a thickened ET if an US is not Available?
ACOG committee opinion number 557, states that all women with AUB do not need to undergo endometrial sampling/biopsy, unless there is high risk of hyperplasia or malignancy. If an US is unavailable, then the committee recommended endometrial biopsy in women with AUB aged 45 years or more and in women < 45 years, in cases of anovulatory AUB (cases of PCOD, Obesity and Diabetes etc.); when they do not respond to conservative treatment.
Premenopausal AUB (Abnormal uterine bleeding) in women that does not respond to treatment should be biopsied when the endometrium is > 11 mm. The pathologic biopsy will show if the lining is too thick (too much estradiol or too little progesterone), or bleeding because it is too thin (raw) which means too little Estradiol and or too much progesterone. Sometimes the bleeding is from a polyp or a fibroid which would require more than a biopsy in the office and a D&C is scheduled.
Most of our patients have normal ultrasounds when they start treatment and often have normal pathology after treatment with estradiol, progesterone and Testosterone pellets.
This document contains is the basis of our use of vaginal ultrasound both before our patients start HRT and during the time they are taking estradiol pellets if they develop postmenopausal bleeding that is unresponsive to our hormone therapy. At BioBalance Health® we take all precautions with our patients so we don’t complicate any pathology that is pre-existing when they first come to our practice. A vaginal ultrasound is the best method of ruling out endometrial cancer and precancer (2 conditions that should not receive estradiol replacement). We also want to discover any existing pathology (fibroids, polyps, ovarian masses) that need the attention of a woman’s gynecologist before they start HRT with estradiol pellets. We want to know what diagnoses we must address when we are taking care of individual patients, and we aspire to “do no harm” while trying to make improve the health and quality of life of our patients.
Source:
ACOG Committee Opinion #734, May 2018. The Role of Transvaginal Ultrasound Evaluating the Endometrium of Women with Post Menopausal Bleeding
This Health cast was written and presented by Dr. Kathy Maupin, M.D., Bio-identical Hormone Replacement Expert and Author. www.BioBalanceHealth.com • (314) 993-0963. Please subscribe to our YouTube channel and please check “ Like “. Follow us on Facebook and Instagram at BioBalanceHealth.
